

Introduction. Mutations in genes encoding the metabolic enzymes isocitrate dehydrogenase (IDH) 1 and 2 are found in 10-20% of patients with acute myeloid leukemia (AML). Recently, IDH inhibitors have shown good clinical response in patient's refractory to standard treatments, providing evidence for a new treatment paradigm. Comprehensive real-world studies are needed to explore genotype-to-phenotype correlations and prognosis of IDH mutated AML, which may influence targeted treatment strategies.
Patients. From a retrospective, European, real-word population (ClinicalTrials.gov Identifier: NCT04369287) we studied 477 IDH mutated patients and 954 IDH wild type patients matched for age, sex and type of treatment with a 1:2 ratio.
Results. Median age of IDH mutated patients was 67 years; IDH1 mutations were found in 202 patients (89% carried R132 mutation), while IDH2 mutations were found in 275 cases (51% and 28% carried R140 and R172 mutations, respectively).
At diagnosis, IDH mutated patients had lower neutrophil and higher platelet count and higher percentage of marrow blasts (P<0.001). IDH mutations were more frequently observed in de novo AML vs. AML from previous myeloid malignancy (P=0.043).
Considering cytogenetic risk according to ELN criteria, the great majority of IDH1 and IDH2 mutated patients had an intermediate cytogenetic risk (84% and 86%, respectively, P<.001, most of them showing a normal karyotype). Considering IDH1 vs. IDH2 mutated population, deletion of chromosome 7 was more frequently reported in IDH2 mutated patients (P=.001).
We then analysed the most common co-mutational patterns in IDH mutated patients. A total of 53% of IDH1 mutated patients carried NPM1 mutations (without FLT3 mutations), while the majority of IDH2 mutated patients had wild type NPM1 gene (P<.001). IDH2 mutated patients more frequently presented with co-mutation in FLT3 gene (P<.001); among IDH2/FLT3 co-mutated patients, the great majority of cases carried the R140 mutation (P<.001). ASXL1 mutations were also more frequently associated with IDH2 mutations (P=.029). Most patients with CEBPA biallelic mutations carried IDH1 or 2 mutations (66%, P=.01), while core binding factor translocations, and mutations in TP53 and RUNX1 were rarely associated with IDH1 or 2 mutations.
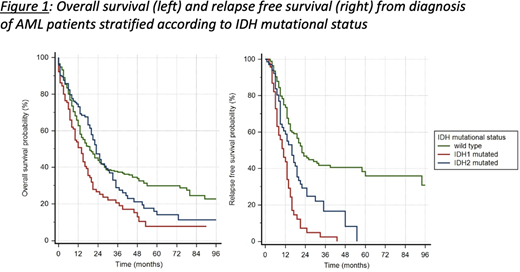
Median overall survival from diagnosis (OS) was 14 months for IDH1 mutated patients, 23 for IDH2 mutated patients and 19 for IDH wild type patients (P<.001, figure 1); the independent negative effect on OS for IDH1 mutations was confirmed in a multivariable analysis on the whole study population including age, sex, ELN risk group, and type of treatment as covariates (HR was 1.65 vs. wild type population and 1.36 vs. IDH2 mutated patients, P<.001), as well as in a specific analysis focused on patients belonging to intermediate ELN risk category (HR 1.75 vs. wild type population, P<.001). Focusing on different mutational hotspots, survival analysis confirmed that IDH1 R132 mutation was associated with worse prognosis among IDH mutated patients (P<.001). Moreover, we observed a reduced relapse-free survival (RFS) for both IDH1 and 2 mutated patients vs. wild type patients (P<.001, figure 1). Multivariable analysis confirmed worse RFS for IDH1 and 2 patients vs. wild type patients (HR 3.8 and 1.4, respectively, P<.001), as well as for IDH1 vs. IDH2 mutated patients (HR 1.5, P<.001).
IDH mutated patients receiving hypomethylating agents (n=211) had a lower response rate vs. wild type patients (56% vs. 36% of treatment failure, respectively, P=.04), while no significant different probability of response to intensive chemotherapy was noticed. In patients who received allogeneic transplantation (n=345), IDH1 mutated patients shower higher relapse rate vs. wild type and IDH2 mutated patients (53% vs. 34%, P<.001).
Conclusion. In a real world context, AML patients with IDH1 and 2 mutations have high marrow blasts percentage, frequently present normal karyotype and show specific co-mutational patterns with respect to NPM1, FLT3 and ASXL1 genes. IDH1 mutations were an independent predictor of unfavorable outcome with high rate of disease recurrence under currently available treatment options, and could be considered as an additional marker to improve personalized prognostic assessment within ELN risk groups. Dissection of prognosis of IDH mutated AML may influence targeted treatment strategies in clinical practice.
Voso:Bristol Myers Squibb: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding. Heibl:Takeda: Honoraria; AOP orphan: Consultancy, Honoraria, Research Funding; BMS/celgene: Consultancy, Honoraria, Research Funding; novartis: Consultancy, Honoraria. Metzeler:Astellas: Honoraria; Daiichi Sankyo: Honoraria; Otsuka Pharma: Consultancy; Pfizer: Consultancy; Jazz Pharmaceuticals: Consultancy; Novartis: Consultancy; Celgene: Consultancy, Honoraria, Research Funding. Thiede:AgenDix GmbH: Other: Co-owner and CEO. Fracchiolla:ABBVIE: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel, accommodations, expenses; Gilead: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel, accommodations, expenses, Speakers Bureau; Pfizer: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel, accommodations, expenses, Speakers Bureau; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel, accommodations, expenses, Speakers Bureau. Todisco:Jannsen, Abbvie, Jazz: Membership on an entity's Board of Directors or advisory committees. Passamonti:Novartis: Speakers Bureau; BMS: Speakers Bureau; Roche: Other: Support of parent study and funding of editorial support.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal